Free Practice Questions for the NCC C-EFM EFM Exam (2026 Updated)
At Marks4sure, we are dedicated to providing IT professionals with the most accurate and reliable preparation materials for the NCC EFM exam. To support your certification journey, we have made a selection of our premium 2026 C-EFM practice questions and answers available completely free. You can take this practice test as many times as you need. Every question includes a detailed, expertly verified explanation to ensure you fully grasp the core security concepts before test day.
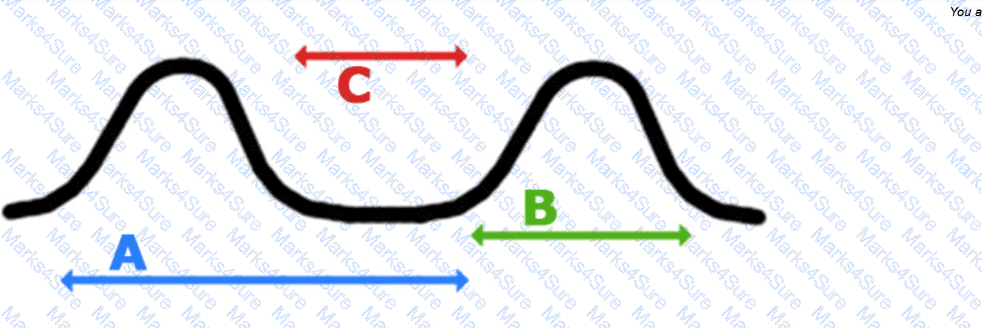
A key differentiating factor when determining if a deceleration is early or late is the
This tracing has lasted for 20 minutes in a woman who is 6 cm dilated. The most appropriate intervention is:
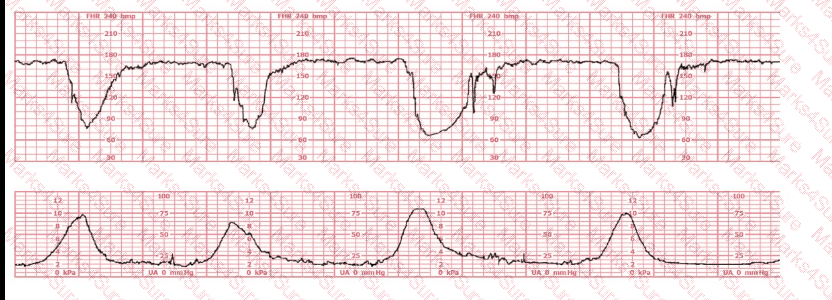
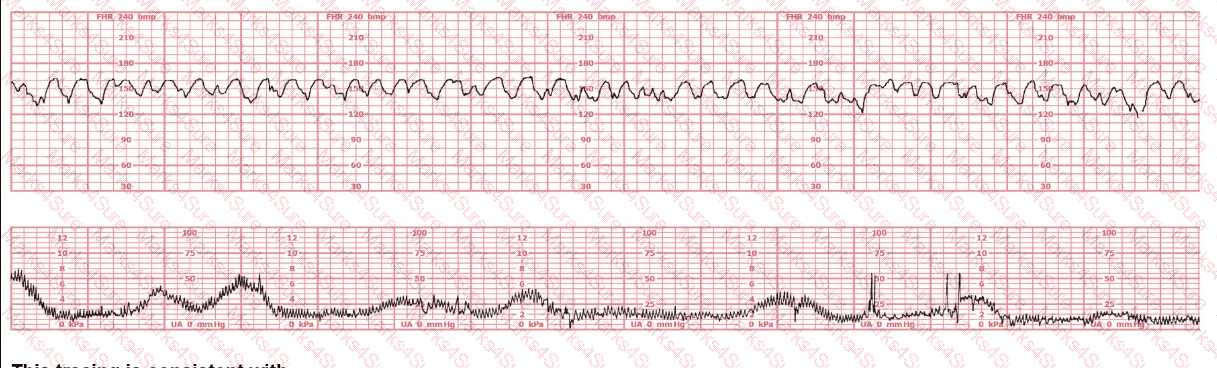
A woman at 38-weeks gestation is admitted to labor and delivery following a fall down the stairs three hours ago. She started feeling contractions in the ambulance. The fetal heart rate tracing shown is on initial evaluation and represents 25 minutes. This tracing is most consistent with a
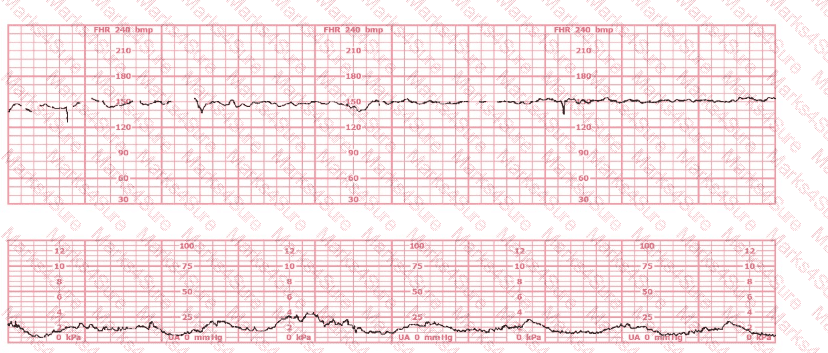
A fetus displays a baseline heart rate of 125 beats per minute with moderate variability. During a contraction, the baseline rate drops abruptly to 80 beats per minute with gradual return to baseline over 90 seconds. This is classified as:
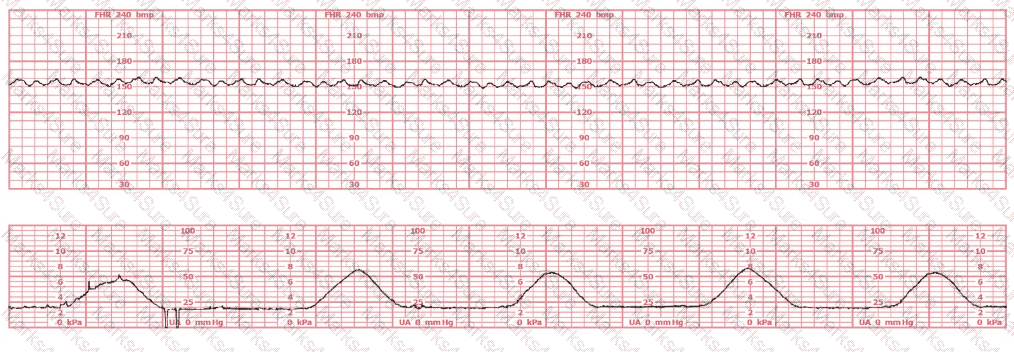
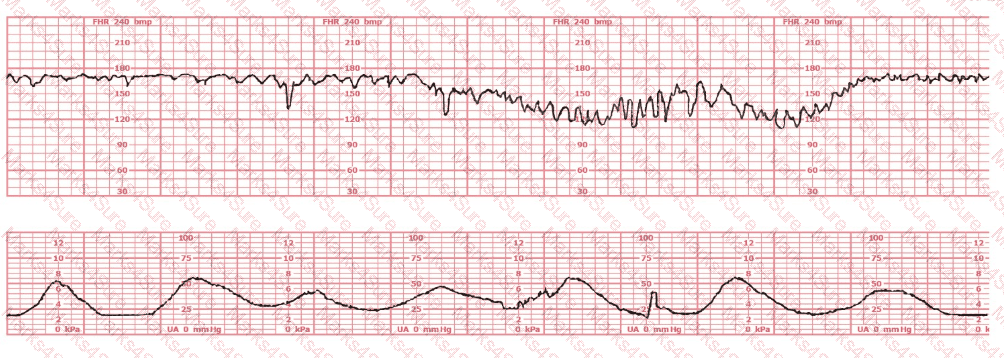
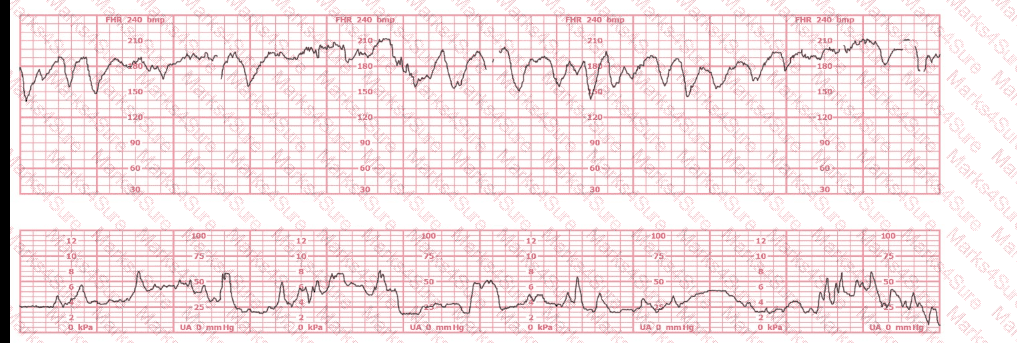
The decelerations seen in the fetal monitoring tracing shown are best described as:
During amnioinfusion, the infusion should be stopped periodically to assess changes in:
A woman is admitted at 41-weeks gestation for fetal evaluation following a motor vehicle accident. She reports that she hit her abdomen on the steering wheel. The underlying physiology of the tracing is most likely:
A woman (G1P0) arrives in triage with a pain score of 4/10 at 39-weeks gestation. The fetal heart rate tracing shown is obtained. The best intervention is to:
The baseline fetal heart rate decreases with gestational age as a result of an increase in:
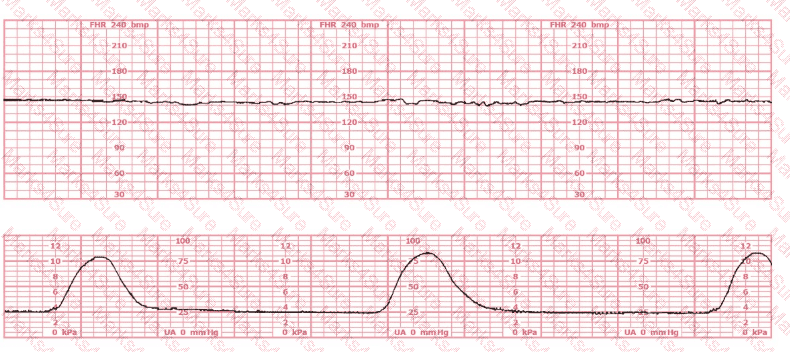
A fetal heart rate pattern shows no accelerations or decelerations. It would be interpreted as a Category II pattern if it occurred with:
When documenting the occurrence of late decelerations in the medical record, what should be charted?
Usually, the duration of an early deceleration in comparison with the contraction is:
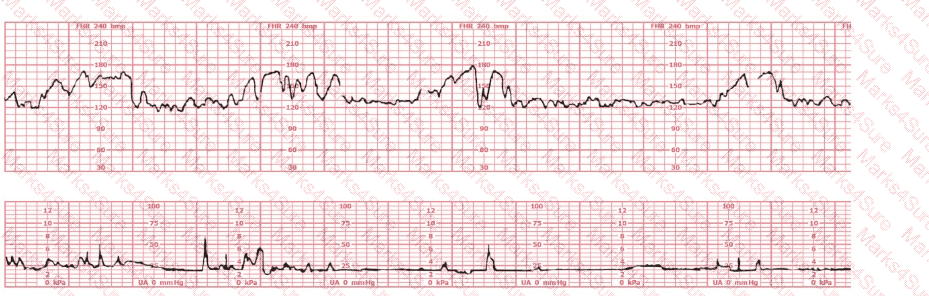
This fetal heart rate tracing is of a woman in labor with dichorionic-diamniotic twins at 36-weeks gestation, 4 cm dilated. She is on oxygen via face mask. Based on the fetal heart rate tracing, what is the most appropriate action?
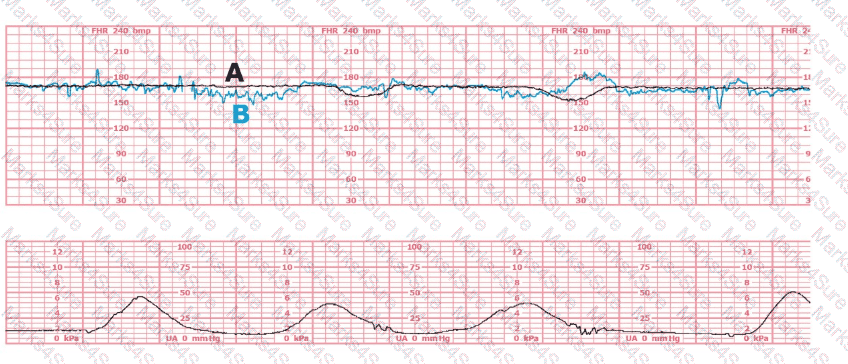
(Tracing A = black; Tracing B = blue)
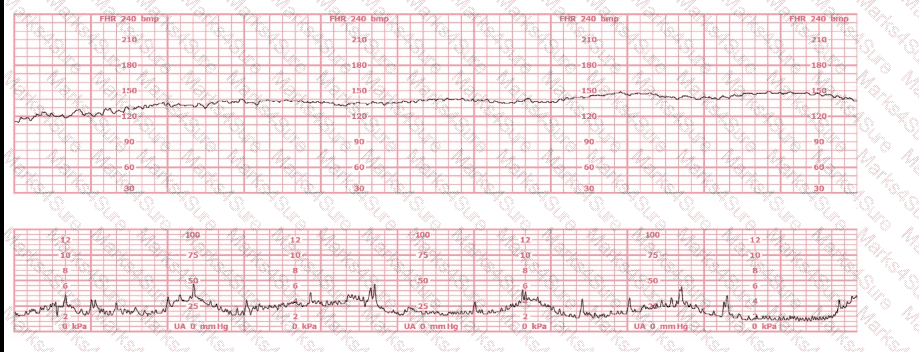
A woman (G1, P0) at 41-weeks gestation presents to OB triage to rule out labor. Her cervical exam is 1 cm/50%/-2. Membranes are intact. She would like to go home if not in labor. Based on this tracing, which represents the last two hours, the best approach is:
To differentiate a fetal dysrhythmia from artifact, it is important to recognize that artifact appears as deflections that are:
A fetal heart rate tracing is abnormal. A change in maternal position and oxygen administration do not correct the pattern. Following birth, a fetal cord blood sample is taken:
pH = 7.25
PaCO₂ = 46 mm Hg
PaO₂ = 20 mm Hg
HCO₃ = 22 mEq/L
Base deficit = –4 mEq/L
These results are best interpreted as:
This external tracing is from a 19-year-old (G1P0) at 39-weeks gestation. She is 6 cm dilated, 100% effaced, and –2 station. The fetus is in an occiput posterior position. She rates her pain as 8. She reports being lightheaded. She is most likely at risk for respiratory:
Nonstress testing is used more frequently for antepartum testing than contraction stress testing because contraction stress testing has a:
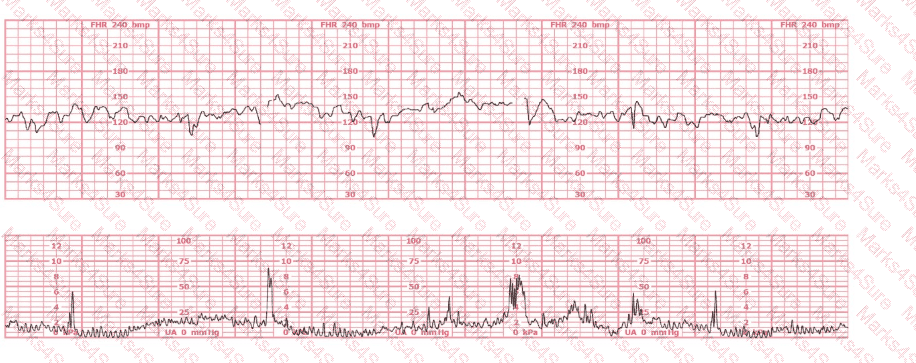
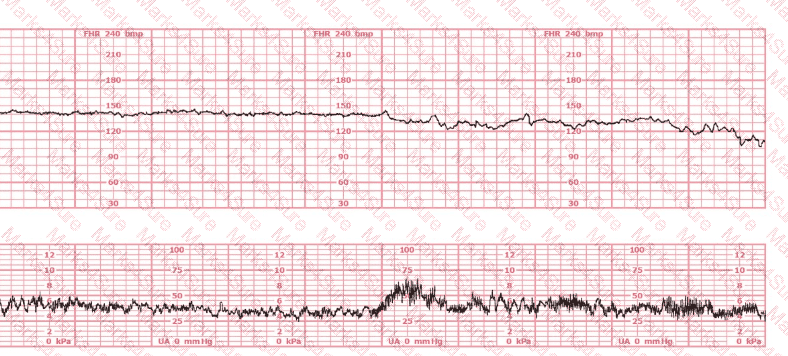
The decelerations seen in the fetal monitoring tracing shown are best described as:
PDF + Testing Engine

Testing Engine
PDF (Q&A)
