Free Practice Questions for the AAPC Certified Professional Coder CPC Exam (2026 Updated)
At Marks4sure, we are dedicated to providing IT professionals with the most accurate and reliable preparation materials for the AAPC CPC exam. To support your certification journey, we have made a selection of our premium 2026 Certified Professional Coder practice questions and answers available completely free. You can take this practice test as many times as you need. Every question includes a detailed, expertly verified explanation to ensure you fully grasp the core security concepts before test day.
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
Which CPT® and ICD-10-CM codes are reported for this procedure?
A 20-year-old female is being seen for the first time by a primary care physician to have a yearly physical. During the examination for the physical, the provider discovers non-inflammed lesions on her legs and arms. The physician performs a complete physical and additional separate documentation for the treatment of the lesions on the bilateral upper and lower extremities. The provider has the patient buy an over-the-counter ointment and will continue to watch them.
What CPT® coding is reported for this visit?
Dr. Carter sees Mrs. White at the Spring Valley Nursing Facility. He saw her last month after she was admitted to the facility. Today is a follow up visit. She is doing well. He documented a medically appropriate history and exam. The patient has osteoporosis, hypertension, dementia. CAD, CHF, and type 2 diabetes (moderate number and complexity of problems). He reviews 4 labs and a telemetry (Moderate data). He adds a Cardizem prescription for better control of her blood pressure which is a moderate risk. What CPT® code does Dr. Carter report for the visit?
A 1-year-old patient has bilateral supernumerary digits:
Left digit contains bone and joint → amputated
Right digit is a soft-tissue nubbin → simple excision
What CPT® coding is reported?
A 45-year-old male, with no prior history of heart disease, has been diagnosed having atherosclerotic heart disease with unstable angina. He is in the cardiologist ' s office for a cardiac MRI test
to determine the morphology and function of his heart under stress. First images obtained are without contrast and then contrast is administered for the next set of images. Then the physician
injects medicine to increase the heart rate and checks the coronary arteries for narrowing or blockage. Physician interprets the test and the results and images are in the medical record.
What radiology CPT® and ICD-10-CM codes are reported?
A 45-year-old female presents to the ED with chest pain. The provider has an Albumin Cobalt Binding Test to determine if the chest pain is ischemic in nature.
That lab test is reported?
A 63-year-old is seen by his. primary care physician for an annual exam. His last exam with the primary care physician was four years ago. He has no complaints.
What CPT code is reported?
A patient receives 200 mg IM Depo-Testosterone.
What HCPCS Level II coding is reported?
A planned partial meniscectomy of the temporomandibular joint is cancelled after anesthesia and incision due to respiratory distress.
What CPT® coding is reported for the oral surgeon?
(A trauma patient needs the following imaging:2 views nasal bones,3 views chest,2 views left forearm,2 views tibia/fibula. To exclude stroke, aCTA head with contrastis also ordered. What CPT® coding is reported?)
A patient is diagnosed with sepsis and associated acute respiratory failure.
What ICD-10-CM code selection is reported?
According to the ICD-10-CM Guidelines, what code is reported as an additional code when the blood pressure of a patient with hypertension remains above goal in spite of the use of antihypertensive medications?
A patient is going to have placement of a myringotomy tube. This tube is placed in the ______ to drain excess fluid.
A patient presents with 26 skin tags on the neck and shoulder. The provider removes all using a scissoring technique.
What CPT® coding is reported?
(A provider documents “pericarditis with effusion” in the assessment. Based on medical terminology, which structure is inflamed?)
A 65-year-old man had a right axillary block by the anesthesiologist. When the arm was totally numb, the arm was prepped and draped, and the surgeon performed tendon repairs of the right first, second, and third fingers. The anesthesiologist monitored the patient throughout the case.
What anesthesia code is reported?
Dr. Burns sees newborn baby James at the birthing center on the same day after the cesarean delivery. Dr. Burns examined baby James, the maternal and newborn history, ordered appropriate blood test tests and hearing screening. He met with the family at the end of the exam.
How would Dr. Bums report his services?
(Patient with erectile dysfunction is presenting for a penile implant. Anon-inflatable penile prosthesisis inserted. What CPT® code is reported for this service?)
A 62-year-old with ventricular fibrillation comes to the outpatient surgery department for the replacement of a pacing cardioverter-defibrillator. The procedure is performed under MAC
anesthesia. The Certified Registered Nurse Anesthetist (CRNA), is working independently without medical direction.
What CPT® and ICD-10-CM codes are reported for the CRNA?
What is the medical term for a procedure that creates a connection between the gallbladder and the small intestine?
Refer to the supplemental information when answering this question:
View MR 903096
What CPT® and ICD-10-CM coding is reported?
A patient presents to the office with dysuria and lower abdominal pain. The physician suspects she has a UTI. A non-automated urinalysis is done in the office and is negative. UTI is ruled out
for the final diagnosis.
What CPT and ICD-10-CM codes are reported?
Multiple laceration repairs were performed:
Simple: cheek (2.5 cm), nose (3 cm)
Intermediate: left leg (9 cm), right leg (11.5 cm)
Complex: left upper arm (4 cm)
What CPT® codes are reported?
(A 45-year-old patient has a history of chronic otitis media in the left ear. The otolaryngologist performs atympanoplastyand doesnot remove the mastoidto repair the patient’s perforated tympanic membrane.What CPT® and ICD-10-CM codes are reported?)
Preoperative diagnosis: Right thigh benign congenital hairy nevus. *1
Postoperative diagnosis: Right thigh benign congenital hairy 0 nevus.
Operation performed: Excision of right thigh benign congenital > 1
nevus, excision size with margins 4.5 cm and closure size 5 cm.
Anesthesia: General.0
Intraoperative antibiotics: Ancef.0
Indications: The patient is a 5-year-old girl who presented with her parents for evaluation of her right thigh congenital nevus. It has been followed by pediatrics and thought to have changed over the past year. Family requested excision. They understood the risks involved, which included but were not limited to risks of general
anesthesia, infection, bleeding, wound dehiscence, and poor scar formation. They understood the scar would likely widen as the child grows because of the location of it and because of the age of the patient. They consented to proceed.
Description of procedure: The patient was seen preoperatively in > I the holding area, identified, and then brought to the operating room. Once adequate general anesthesia had been induced, the patient ' s right thigh was prepped and draped in standard surgical fashion. An elliptical excision measuring 6 x 1.8 cm had been marked. This was injected with Lidocaine with epinephrine, total of 6 cc of 1% with 1:100,000. After an adequate amount of time, a #15 blade was used to sharply excise this full thickness.
This was passed to pathology for review. The wound required □ limited undermining in the deep subcutaneous plane on both sides for approximately 1.5 cm in order to allow mobilization of the skin for closure. The skin was then closed in a layered fashion using 3-0 Vicryl on the dermis and then 4-0 Monocryl running subcuticular in the skin, the wound was cleaned and dressed with Dermabond and Steri-Strips.
The patient was then cleaned and turned over to anesthesia for S extubation.
She was extubated successfully in the operating room and taken S to the recovery room in stable condition. There were no complications.
What CPT® and ICD-10-CM codes are reported?
(Day 1: Provider admits patient toobservation carefor type 2 diabetes with hyperglycemia, orders labs, consults endocrinologist, starts IV insulin drip, keeps overnight. Day 2: orders glucose test, dietitian, documents total time 25 minutes. Day 3: glucose normal, documents 15 minutes, discharges patient. What E/M coding is reported by the physician for the patient in observation care?)
A patient presents to the labor and delivery department for a planned cesarean section for triplets. She is at 37 weeks gestation. She is given a continuous epidural for the delivery.
What anesthesia coding is reported?
Repeat three-view imaging of both hips and pelvis is performed on the same day due to a new fall, interpreted by the same radiologist.
What CPT® coding is reported?
A patient has chronic cholesteatoma in the right middle ear. The otolaryngologist performed a tympanoplasty with a radical mastoidectomy, removing the middle ear cholesteatoma. Grafting
technique was used to repair the eardrum with ossicular chain reconstruction.
What CPT® code is reported for this surgery?
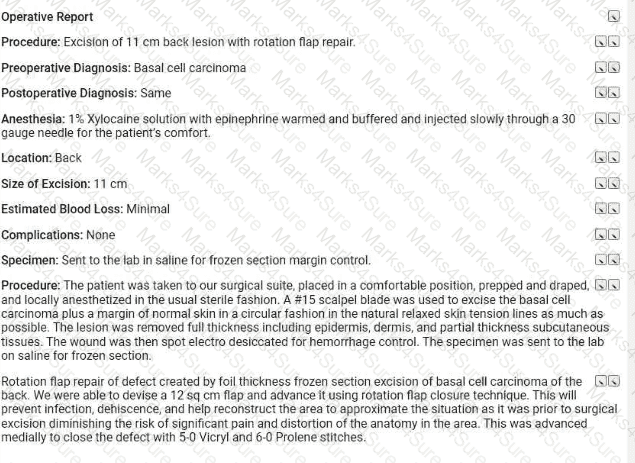
(Full Case:Procedure:Excision of6.0 cm malignant lesionof theright forearmwithadjacent tissue transferusing arotation flap.Pre/Post-op Dx:Basal cell carcinoma, right forearm.Anesthesia:local (1% Xylocaine with epi).Defect size:8 sq cm.Specimen:sent forfrozen section margin control; margins confirmed clear.Closure:rotation flap from adjacent healthy tissue,total area 8 sq cm, secured with layered closure (5-0 Vicryl/6-0 Prolene).Question:What CPT® coding is reported?)
Which one of the following is correct to report an intermediate repair code (12031–12037)?
(From the left femoral artery, the catheter was advanced into the abdominal aorta, andaortographywas performed to view the location of the left inferior phrenic artery. Next the catheter was advanced into theleft inferior phrenicand into theleft superior suprarenal (adrenal) arteryand angiography was performed. The angiography showed no blockage of the left adrenal artery. What CPT® codes are reported?)
A 57-year-old woman with a physical status of 3 received general endotracheal anesthesia for a panniculectomy. The anesthesiologist personally performed the entire anesthesia service.
What CPT@ coding is reported for the anesthesia?
A 52-year-old woman has been experiencing discomfort and itching In the vulvar area for several months. She has a history of abnormal Pap smears and a recent biopsy revealed vulvar intraepithelial neoplasia (VIN III). Decision has been made to perform a vulvectomy.
Procedure: Under general anesthesia, the surgeon made an incision in the vulvar area and removed the vulva (more than 80%), including the affected skin and deep subcutaneous tissue.
What CPT® and ICD-10-CM codes are reported?
A surgeon performs a complete bilateral mastectomy with insertion of breast prosthesis at the same surgical session.
What CPT@ coding is reported?
A 42-year-old male is diagnosed with a left renal mass. Patient is placed under general anesthesia and in prone position. A periumbilical incision is made and a trocar inserted. A laparoscope is inserted and advanced to the operative site. The left kidney is removed, along with part of the left ureter. What CPT® code is reported for this procedure?
View MR 007400
MR 007400
Radiology Report
Patient: J. Lowe Date of Service: 06/10/XX
Age: 45
MR#: 4589799
Account #: 3216770
Location: ABC Imaging Center
Study: Mammogram bilateral screening, all views, producing direct digital image
Reason: Screen
Bilateral digital mammography with computer-aided detection (CAD)
No previous mammograms are available for comparison.
Clinical history: The patient has a positive family history (mother and sister) of breast cancer.
Mammogram was read with the assistance of GE iCAD (computerized diagnostic) system.
Findings: No dominant speculated mass or suspicious area of clustered pleomorphic microcalcifications is apparent Skin and nipples are seen to be normal. The axilla are unremarkable.
What CPT® coding is reported for this case?
Refer to the supplemental information when answering this question:
View MR 004813
What CPT® and ICD-10-CM codes are reported?
(A provider orders a liquid chromatography mass spectrometry (LC-MS) definitive drug test for a patient suspected ofacetaminophen (analgesic) overdose. What CPT® code is reported for the test?)
A patient ' s left eye is damaged beyond repair due to a work injury. The provider fabricates a prosthesis from silicon materials and makes modifications to restore the patient ' s cosmetic appearance.
What CPT® code is reported?
A 60-year-old male suffering from degenerative disc disease at the L3-L4 and L5-S1 levels was placed under general anesthesia. Using an anterior approach, the L3-L4 disc space was exposed. Using blunt dissection, the disc space was cleaned. The disc space was then sized and trialed. Excellent placement and insertion of the artificial disc at L3-L4 was noted. The area was inspected and there was no compression of any nerve roots. Same procedure was performed on L5-S1 level. Peritoneum was then allowed to return to normal anatomic position and entire area was copiously irrigated. The wound was closed in a layered fashion. The patient tolerated the discectomy and arthroplasty well and was returned to recovery in good condition. What CPT® coding is reported for this procedure?
A 5-year-old patient has a fractured radius. The orthopedist provides moderate sedation and the reduction. The time is documented as 21 minutes.
What CPT® code is reported for the moderate sedation?
A patient comes to the gynecologist ' s office to check if she is pregnant. A urine sample is taken and tested. The visual result is positive that she is pregnant.
What CPT® code is reported '
(A 6-month-old child was brought to the hospital with severe breathing difficulties. After testing, the child was diagnosed withtracheal stenosis present from birth. The pediatric surgeon performed atracheoplasty(surgical widening of the trachea). What CPT® and ICD-10-CM codes are reported?)
A patient with malignant lymphoma is administered the antineoplastic drug Rituximab 800 mg and then 100 mg of Benadryl.
Which HCPCS Level II codes are reported for both drugs administered intravenously?
A 6-French sheath and catheter is placed into the coronary artery and is advanced to the left side of the heart into the ventricle. Ventriculography is performed using power injection of contrast agent. Pressures in the left heart are obtained. The coronary arteries are also selected and imaged.
What CPT® code is reported?
According to the ICD-10-CM coding guidelines, when coding hypertension with heart conditions classified to I50.- or I51.4–I51.7, I51.89, I51.9, what category should be used?
A 65-year-old gentleman presents for refill of medications and follow-up for his chronic conditions. The patient indicates good medicine compliance. No new symptoms or complaints.
Appropriate history and exam are obtained. Labs that were ordered from previous visit were reviewed and discussed with patient. The following are the diagnoses and treatment:
Hypokalemia - stable. Refill Potassium 20 MEQ
Hypertension - blood pressure remaining stable. Patient states home readings have been in line with goals. Refill prescription Lisinopril.
Esophageal Reflux - Patient denies any new symptoms. Stable condition. Continue taking over the counter Prevacid oral capsules, 1 every day.
Patient is instructed to follow up in 3 months. Labs will be obtained prior to visit.
What CPT® code is reported?
A comatose patient is seen in the ER. The patient has a history of depression. Drug testing confirm she overdosed on tricyclic antidepressant drugs doxepin, amoxapine, and clomipramine.
What CPT® code is reported?
A patient had surgery a year ago to repair two flexor tendons in his forearm. He is in surgery for a secondary repair for the same two tendons.
Which CPT® coding is reported?
A 67-year-old patient has osteomyelitis of the shoulder blade and is in surgery to remove the sequestered section of dead infected fragment bone from surrounding bone.
What CPT® code is reported?
Mr. Woolridge has had a suspicious lesion on his left shoulder for approximately eight weeks that is not healing. On the dermatologist ' s exam of left shoulder blade, there is excoriation and scabbing and the lesion not healing. Patient agrees and wishes to proceed with a punch biopsy of the lesion. A punch biopsy is taken of the lesion and sent to pathology. A simple repair is performed at the biopsy site.
What CPT® and ICD-10-CM codes are reported?
A patient who has HIV disease presents with loin pain in the clinic today. The patient reports he is having trouble sleeping due to the pain. What ICD-10-CM coding is reported?
A patient has nausea with several episodes of emesis along with severe stomach pain due to dehydration. Normal saline is infused in the same bag with 2 mg ondansetron to help with the
nausea. Then a dose of 15 mg ketorolac tromethamine was given for the stomach pain.
What J codes are reported for these services?
(An orthopedic surgeon evaluated a patient in the emergency room two months after a surgical repair of a right radius and ulnar shaft fracture. After reinjury, imaging shows a displaced proximal fixation screw andmalunion of only the radial shaft. The same surgeon performs surgery to repair the malunion using a graft from the hip. What CPT® and diagnosis codes are reported?)
The CPT® code book provides full descriptions of medical procedures, although some descriptions require the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 69644?
View MR 099405
MR 099405
CC: Shortness of breath
HPI: 16-year-old female comes into the ED for shortness of breath for the last two days. She is an asthmatic.
Current medications being used to treat symptoms is Advair, which is not working and breathing is getting worse. Does not feel that Advair has been helping. Patient tried Albuterol for persistent coughing, is not helping. Coughing 10-15 minutes at a time. Patient has used the Albuterol 3x in the last 16 hrs. ED physician admits her to observation status.
ROS: No fever, no headache. No purulent discharge from the eyes. No earache. No nasal discharge or sore throat. No swollen glands in the neck. No palpitations. Dyspnea and cough. Some chest pain. No nausea or vomiting. No abdominal pain, diarrhea, or constipation.
PMH: Asthma
SH: Lives with both parents.
FH: Family hx of asthma, paternal side
ALLERGIES: PCN-200 CAPS. Allergies have been reviewed with child’s family and no changes reported.
PE: General appearance: normal, alert. Talks in sentences. Pink lips and cheeks. Oriented. Well developed. Well nourished. Well hydrated.
Eyes: normal. External eye: no hyperemia of the conjunctiva. No discharge from the conjunctiva
Ears: general/bilateral. TM: normal. Nose: rhinorrhea. Pharynx/Oropharynx: normal. Neck: normal.
Lymph nodes: normal.
Lungs: before Albuterol neb, mode air entry b/l. No rales, rhonchi or wheezes. After Albuterol neb. improvement of air entry b/l. Respiratory movements were normal. No intercostals inspiratory retraction was observed.
Cardiovascular system: normal. Heart rate and rhythm normal. Heart sounds normal. No murmurs were heard.
GI: abdomen normal with no tenderness or masses. Normal bowel sounds. No hepatosplenomegaly
Skin: normal warm and dry. Pink well perfused
Musculoskeletal system patient indicates lower to mid back pain when she lies down on her back and when she rolls over. No CVA tenderness.
Assessment: Asthma, acute exacerbation
Plan: Will keep her in observation overnight. Will administer oral steroids and breathing treatment. CXR ordered and to be taken in the morning.
What E/M code is reported?
A patient with suspected gynecologic malignancy undergoes laparoscopic staging including bilateral pelvic lymphadenectomy, periaortic lymph node sampling, peritoneal washings, peritoneal and diaphragmatic biopsies, and omentectomy.
What CPT® coding is reported?
(A 1-year-old patient was born with twosupernumerary digits, one extending from the right pinky and one extending from the left pinky. The digit from his left pinky is larger and includes themetacarpal bone with a jointand is amputated. The one on the right is anubbinand containsno bony structure. The hand surgeon removes the extra digit containingsoft tissueby a simple excision. What is the CPT® coding for the procedures performed?)
Which one of the following is an example of a case in which a diabetes-related problem exists and the code for diabetes is never sequenced first?
A diagnostic mammogram is performed on the left and right breasts. Computer-aided detection is also used to further analyze the image for possible lesions.
What CPT® coding is reported for this radiology service?
Which circumstance supports medical necessity for a payment by the insurance company?
(What is the ICD-10-CM code for amedial meniscus tearof theleft kneedue to arecent football injury?)
A physician orders a CT scan of the abdomen without contrast.
What CPT® coding is reported?
A business requires drug testing for cocaine and methamphetamines prior to hiring a job candidate. A single analysis with direct optical observation is performed, followed by a confirmation for cocaine.
Which codes are used for reporting the testing and confirmation?
A patient presents with keratosis lesions on her left cheek, above the left eyebrow, and on the chin area. The dermatologist treats those areas by lightly sanding the surface of a total of 5 lesions.
What CPT® coding is reported?
(A driver crashes into a guardrail and sustains a fracture of the anterior fossa cranial base with involvement of thesphenoid sinus, withno CSF leak. The patient undergoessurgical nasal sinus endoscopy with sphenoidotomyto evaluate and treat the sinus injury. No CSF leak repair is performed. What is the correct procedure and diagnosis coding combination to report this service?)
A 30-year-old patient with a scalp defect is having plastic surgery to insert tissue expanders. The provider inserts the implants, closes the skin, and increases the volume of the expanders by injecting saline solution. Tissue is expanded until a satisfactory aesthetic outcome is obtained to repair the scalp defect.
What CPT® code is reported?
An ED provider evaluates a patient with NSTEMI, consults cardiology, and the patient is admitted for PCI.
What E/M service and ICD-10-CM coding is reported by the ED provider?
(A patient training for a marathon collapsed due to heat exhaustion on a very hot day and is treated at a nonfacility urgent care center. The physician diagnoses heat exhaustion and dehydration and begins IV therapy of normal saline (pre-packaged fluid and electrolytes). The hydration lasts1 hour and 30 minutes. What CPT® coding is reported?)
A patient is diagnosed with a pressure ulcer on her right heel that is currently being treated.
What ICD-10-CM code is reported?
View MR 099407
MR 099407
Emergency Department Visit
Chief Complaint: VOMITING.
This started just prior to arrival and is still present. He has had nausea and vomiting. No diarrhea, black stools, bloody stools or abdominal pain. Pt is diabetic and has been having elevated blood sugars (320 mg/dL).
REVIEW OF SYSTEMS: Unobtainable due to patient ' s altered mental status.
PAST HISTORY: Poorly controlled diabetes mellitus, with history of poor compliance.
Medications: See Nurses Notes.
Allergies: PCN.
SOCIAL HISTORY: Nonsmoker. No alcohol use or drug use.
ADDITIONAL NOTES: The nursing notes have been reviewed.
PHYSICAL EXAM
Appearance: Lethargic. Patient in mild distress.
Vital Signs: Have been reviewed-tachycardic.
Eyes: Pupils equal, round and reactive to light.
ENT: Dry mucous membranes present.
Neck: Normal inspection. Neck supple.
CVS: Tachycardia. Heart sounds normal. Pulses normal.
E D. Course: Insulin IV drip per protocol, at 10 units/hr.
Zofran 8 mg 01:33 Jul 13 2008 IVP.
Phenergan 25 mg IVP. 07:52.Discussed case with physician. Dr. X. Reviewed test results. Agreed upon treatment plan. Physician will see patient in hospital.
Total critical care time: 45 min.
Disposition: Admitted to Intensive Care Unit. Condition: stable.
Admit decision based on need for monitoring and IV hydration and medications.
CLINICAL IMPRESSION: Vomiting, diabetic ketoacidosis, probable diabetes insipidus.
What E/M code is reported for this encounter?
A 5-year-old who has an allergy history experienced a possible reaction to peanuts. A quantitative, high-sensitive fluorescent enzyme immunoassay was used to measure specific IgE for recombinant peanut components. Results showed there was no reaction indicating the child has a peanut allergy.
What lab test is reported?
A patient has suspicious lesions on his feet. Biopsies confirm squamous cell carcinoma. The patient elects to destroy a 0.6 cm lesion on the right dorsal foot and a 2.0 cm lesion on the left dorsal foot using cryosurgery.
What CPT® coding is reported?
(A 14-month-old male with a unilateral complete cleft lip and alveolar cleft palate had prior repair of the cleft lip. He now presents forreconstruction of the palatewith closing the fissure in the soft tissue of thealveolar ridge with bone graft. What CPT® coding is reported?)
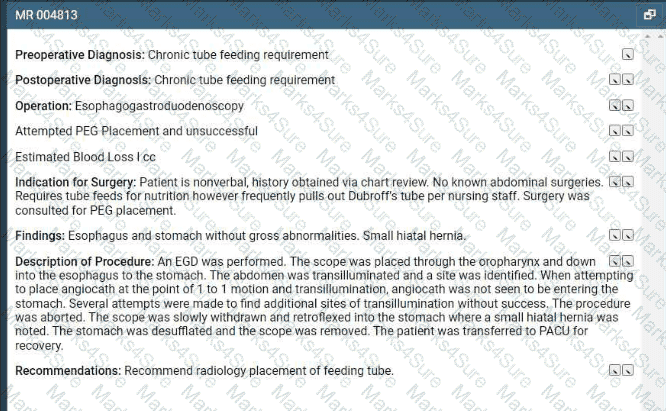
A patient arrives for a PEG placement. The patient requires tube feeds for nutrition but frequently pulls out the dobhoffs tube. An EGD was performed. Several attempts were made to place the
PEG tube without success so the procedure was aborted. During the withdraw of the scope, a small hiatal hernia was noted in the stomach. The scope was removed the the patient transferred
to recovery.
What CPT and ICD-10-CM coding is reported?
A patient with severe diverticulitis in the sigmoid colon presents to surgery for a partial colectomy. The physician performs an exploratory laparoscopic laparotomy to verify the location of the diverticulitis. Once identified, it was noted that there was bleeding from the diverticulitis. The physician transects the descending colon and then transects at the line of the rectum.
The physician mobilizes the splenic flexure in order to create a colostomy with the proximal portion of the remaining colon. The distal portion of the colon is closed. The physician washes the patient ' s abdomen with saline, removes all trocars and instruments, and then closes the abdomen with sutures.
What CPT® and ICD-10-CM codes are reported?
A patient who is 37 weeks ' gestation is admitted to labor and delivery for a cesarean delivery. An external cephalic version was performed successfully several days ago and she now presents in labor, fully dilated, and the fetus has returned to a footling presentation.
What anesthesia code is reported?
An established patient presents with fever and sore throat. Rapid strep test is positive.
What CPT® and ICD-10-CM codes are reported?
Mrs. Wilder presents with right and left leg swelling. Venous thrombosis imaging of each leg is done and shows deep venous embolism and thrombosis in each leg.
What CPT® and ICD-10-CM codes are reported?
During a laparoscopic hemicolectomy, the left kidney is accidentally perforated. A nephrologist performs open repair of the kidney laceration and places a JP drain.
What CPT® and ICD-10-CM coding is reported by the nephrologist?
Four malignant peritoneal tumors are excised, the largest measuring 15 cm.
What CPT® and ICD-10-CM coding is reported?
A healthy 35-year-old undergoes EP study and ablation under general anesthesia.
What anesthesia coding is correct?
Refer to the supplemental information when answering this question:
View MR 623654
What CPTO coding is reported for this case?
(A patient presents with fatigue and unexplained weight gain. To evaluate possible thyroid dysfunction, the provider orders a single laboratory test to measurethyroid-stimulating hormone (TSH). A routine venous blood sample is collected and sent to the laboratory.Which CPT® and ICD-10-CM® codes are reported?)
The patient came in with an inflamed seborrheic keratosis on her nose for a shave removal. After applying local anesthesia, a 0.7 cm dermal lesion was removed using an 11 blade.
What CPT® and ICD-10-CM codes are reported?
(Preoperative diagnoses:Bradycardia.
Postoperative diagnosis:Bradycardia.
Procedure performed:Dual-chamber pacemaker implantation.
Brief history:77-year-old female with recurrent syncope; evaluation revealed first-degree AV block, sinus bradycardia, bundle-branch block; bradyarrhythmia suspected; after discussion with her sister, dual-chamber pacemaker recommended; risks explained; consent obtained.
Procedure details:Taken to cardiac catheterization lab; positioned on cath table; prepped/draped standard; procedure challenging due to agitation despite adequate sedation; left infraclavicular area anesthetized with 0.5 cc Xylocaine; pacemaker pocket created; hemostasis with cautery; 9-French peel-away sheath used to introduce an atrial and a ventricular lead; leads positioned with excellent thresholds; secured with O-silk sutures over sleeves; pulse generator connected; pocket flushed with antibiotic solution; pacemaker/leads placed in pocket; incision closed in two layers; performed under fluoroscopic guidance.
Complication:None.
Plan:Return to recovery; discharge later this evening to nursing home with routine post-pacemaker care.
Question:What CPT® coding is reported for this procedure?)
A 42-year-old male is diagnosed with a left renal mass. Patient is placed under general anesthesia and in prone position. A periumbilical incision is made, and a trocar inserted. A laparoscope is
inserted and advanced to the operative site. The left kidney is partially removed.
What CPT @ code is reported for this procedure?
(A 65-year-old male patient passed away due to unknown causes. An autopsy was ordered by the attending physician to determine the cause of death. The pathologist performed agross and microscopic examination autopsy, that includes thebrain and spinal cord. What CPT® coding is reported?)
(A dermatologist excises abasal celllesion from an area of thescalp, measuring3.7 cm. This is closed with alayered repair. What CPT® and ICD-10-CM codes are reported?)
A patient with a history of a right-hand mass presents for outpatient surgical excision. The surgeon excises the 1.5 cm mass with margins using a scalpel with dissection extending through the dermis into the subcutaneous tissue. Hemostasis is achieved with electrocautery, and the wound is closed. Final pathology confirms the mass is a subcutaneous arteriovenous hemangioma.
Which CPT® and ICD-10-CM codes are reported?
(A wheelchair-bound resident of a skilled nursing facility is seen in the physician’s office. The physician’s office makes arrangements with a social worker to take the patient back to the skilled nursing facility. What is the HCPCS Level II transportation service code?)
A pediatrician removes impacted cerumen using irrigation in the right ear and instrumentation in the left ear.
What CPT® coding is reported?
A patient presents with recurrent spontaneous episodes of dizziness of unclear etiology. Caloric vestibular testing is performed irrigating both ears with warm and cold water while evaluating the patient’s eye movements. There is a total of three irrigations.
What CPT® coding is reported?
The CPT® code book provides full descriptions of medical procedures, with some descriptions requiring the use of a semicolon (;) to distinguish among closely related procedures.
What is the full description of CPT® code 35860?
(The patient presents to the emergency department with chest pain. EKG showsNSTEMIand troponin is abnormal. The ED provider discusses the case with a cardiologist and the patient is admitted for heart catheterization/PCI. What is the E/M service and ICD-10-CM coding reported for the ED provider?)
A patient with abnormal growth had a suppression study that included five glucose tests and five human growth hormone tests.
What CPT@ coding is reported?
A physician excises a 3.5 cm malignant lesion including margins from the back. Then a destruction of a 2.0 cm benign lesion on the right cheek of the face with cryosurgery.
What CPT@ and ICD-10-CM is reported?
A cardiologist performs and interprets a 12-lead ECG in the office.
What CPT® coding is reported?
(A patient arrives with pain due to a chest injury from blunt force. The provider takes X-ray imaging with6 views of the chest. What CPT® coding is reported?)
A patient has a 5 cm tumor in the left lower quadrant abdominal wall, excised through dermis and subcutaneous tissue. Pathology is pending to rule out cancer.
What CPT® and ICD-10-CM codes are reported?
(A patient with abnormal growth had asuppression studythat includedfive glucose testsandfive human growth hormone tests. What CPT® coding is reported?)
An interventional radiologist performs an abdominal paracentesis in his office utilizing ultrasonic imaging guidance to remove excess fluid. What CPT® coding is reported?
(A patient is seen by her podiatrist to treat a painfulleft ingrown toenailon the big toe. The podiatrist performs awedge excisionof the skin of the nail fold at the lateral margin. Local anesthetic is administered, and an elliptical incision is made through subcutaneous tissue of the affected nail groove. A wedge-shaped piece of soft tissue from the nail margins is removed. What CPT® code is reported?)
A 42-year-old with chronic left trochanteric bursitis is scheduled to receive an injection at the Pain Clinic. A 22-gauge spinal needle is introduced into the trochanteric bursa under ultrasonic guidance, and a total volume of 8 cc of normal saline and 40 mg of Kenalog was injected.
What CPT® code should be reported for the surgical procedure?
A 55-year-old patient with suspected liver cancer was seen by the physician to obtain a biopsy. The special biopsy needle was placed using ultrasonic guidance. The physician obtained a small tissue sample from the liver, which was then sent to pathology.
What CPT® codes are reported?
A patient with intermittent asthma with exacerbation undergoes spirometry before and after bronchodilator.
What CPT® and ICD-10-CM codes are reported?
A 45-year-old patient comes In with chronic sinusitis that has not responded to medication. The physician decides to use a sinus stent implant to help alleviate the patients symptoms.
The physician inserts the implant into the ethmoid sinus using a delivery system. This implant is designed to keep the surgical opening clear, prop open the sinus, and gradually release a corticosteroid with anti-inflammatory properties directly to the sinus lining. The implant is not permanent and will dissolve over time.
What HCPCS Level II code is reported?
(Which statement accurately reflects CPT® parenthetical guidance for codes69209and69210?)
Patient is admitted in observation care on 12/2/20XX in the morning for acute asthma exacerbation. The ED physician requires the patient to stay overnight. Next day, 12/3/20XX the patient is
discharged from observation care in the afternoon. Patient ' s total stay in observation was 16 hours.
What E/M categories and code ranges are appropriate to report?
Patient with erectile dysfunction is presenting for same day surgery in removal and replacement of an inflatable penile prosthesis.
What CPT® code is reported for this service?
A 42-year-old male is diagnosed with a left renal mass. An abdominal incision along with rib resection is made to expose and access the kidney. The left kidney is removed, along with surrounding fat, adrenal gland, lymph nodes in the area, and the incision site is sutured. What CPT ® code is reported for this procedure?
Ten-year-old boy has a painful felon abscess of the deep tissues of the palmar surface of his right thumb. The provider makes an incision on one side of the nail and then across the fingertip parallel to the end of the nail. He identifies the area of abscess and drains it. A drainage tube is inserted.
What CPT® and ICD-10-CM is reported?
(Full Case:Patient:V. Bowen.Physician:C.S., MD.Reason for admission:Abdominal pain.HPI:admitted this morning; sudden onset RUQ pain began ~4:00 p.m. yesterday; started while eating; 8/10; chills/sweating/nausea; no vomiting/diarrhea; last BM 2:00 p.m. yesterday; unable to pass stool or gas since; abdominal distention; poor sleep; prior similar episodes relieved by gas tablets but not this time; no discolored stool/urine.PMH:HTN (losartan; missed dose).PSH:bunion surgery right foot.FH:HTN.SH:no smoking/alcohol.Meds:losartan daily.Allergies:NKDA.ROS:nausea, no emesis; no flatus/stool since yesterday; no weight change; no SOB/chest pain; no jaundice; no urinary frequency/urgency.PE:alert/oriented x3; obvious abdominal discomfort. Vitals 139/100, pulse 100, RR 16, temp 36.4. HEENT normal; CV regular; lungs clear. Abdomen: +BS, soft but very tender; worst RUQ;Murphy’s sign; guarding and rebound (worse with palpation). Extremities trace edema.Labs ordered/reviewed:CMP with abnormal LFT/bili; CBC WBC 9.9; etc.Final assessment:RUQ abdominal pain,rule out cholecystitis.Plan:NPO; morphine IV (controlled substance); IV NS 150 cc/hr; abdominal ultrasound and HIDA ordered; consider surgical consult based on results.Question:What CPT® and ICD-10-CM codes are reported?)
(A patient presents for surgery due to recurrent lumbar radiculopathy at a previously operated spinal level. The surgeon performs arepeat exploration laminotomywithbilateral foraminotomyto decompress nerve roots at theL1–L2 interspace. No additional spinal levels are treated. What CPT® coding is reported?)
A patient has squamous cell carcinoma lesions destroyed with cryosurgery:
0.6 cm right dorsal foot
2.0 cm left dorsal foot
What CPT® coding is reported?
A pathologist performs fluorescent microscopy for chromosomal abnormalities, but no specific CPT® code exists.
Which unlisted CPT® code is reported?
A patient was in a car accident as the driver and suffered a concussion with brief loss of consciousness (15 minutes). What ICD-10-CM codes are reported?
A patient with compression fractures of L5 and the sacrum undergoes vertebroplasty, with cement injected into two vertebral bodies, performed bilaterally.
What CPT® coding is reported?
A 55-year-old patient was recently diagnosed with an enlarged goiter. It has been two years since her last visit to the endocrinologist. A new doctor in the exact same specialty group will be examining her. The physician performs a medically appropriate history and exam. The provider reviewed the TSH results and ultrasound. The provider orders a fine needle aspiration biopsy which is a minor procedure.
What E/M code is reported?
An elderly patient comes into the emergency department (ED) with shortness of breath. An ECG is performed The final diagnosis at discharge is impending myocardial infarction.
According to ICD-10-CM guidelines, how is this reported?
Patient has cervical spondylosis with myelopathy. The surgeon performed a bilateral posterior laminectomy with facetectomies at each level and foraminotomies performed between interspaces C5-C6 and C6-C7. Bilateral decompression of the nerve roots is achieved.
What CPT® coding is reported?
(A 5-year-old patient has a fractured radius. The orthopedist providesmoderate sedationand the reduction. The intra-service sedation time is documented as21 minutes. What CPT® code is reported for the moderate sedation?)
(A patient presents for evaluation of suspicious skin lesions. During the encounter, the provider performs:
• Incisional biopsy of adeep inflammatory lesionon the upper arm
• Punch biopsy of aseparate lesionon the forearm
• Shave biopsy of asuperficial lesionon the shoulder
Each biopsy is performed on a separate lesion for diagnostic purposes, and all specimens are submitted to pathology. What CPT® coding is reported?)
PDF + Testing Engine

Testing Engine
PDF (Q&A)
